C2006/F2402 '08 OUTLINE OF LECTURE #22
(c) 2008 Dr. Deborah Mowshowitz, Columbia University, New York, NY. Last update 04/22/2008 09:48 AM . A few minor typos fixed 4/22.
Handouts: Need 22B (Hormones
Overall), 22A (Thyroid,
catecholamines).
This topic is not covered in Becker. It is covered in Sadava/Purves. If you want a
more detailed treatment, any physiology book will do. There are lots of good
physiology books available; the one by Sherwood has been used here for the
last few years. The texts by Vander or by Silverthorn are widely available
and are also quite good. There is an endocrinology book on line through
Pubmed. Go to
books to see the list of books available or to search by topic. Also
don't forget about
Kimball's
biology pages.
I. Homeostatic Control -- The Circuit View (See handout 21B, top.)
The Circuit View of the General Case (Handout 21B) -- A few Critical Points. (Same as II-C of Lecture 21)
1. Circuit = 1 loop of seesaw. Seesaw = double circuit. Often two circuits to make opposite types of corrections.
2. Signals: Signals can be hormonal or neuronal.
3. Afferent vs Efferent Signals. Bottom half of circuit has two arms -- afferent vs efferent
Afferent information goes from sensors → in to IC
Efferent goes out of IC → toward effectors
4. Regulation vs Control.
a. Regulation/regulated variable: The variable (glucose level) you wish to keep at an approximately constant level is said to be "regulated."
b. Control/controlled process: The processes that alter levels of the regulated variable (glucose uptake, release or shivering, sweating, etc.) are said to be "controlled."
c. What's the difference?
The point of the system is to maintain homeostasis of blood glucose levels, internal temperature, etc. Not to maintain homeostasis of rates of glucose uptake, sweating, etc.
The value of the regulated variable stays about the same; the rates of the controlled processes (glucose uptake, heat loss, heat generation, etc. ) can vary as much as necessary to achieve homeostasis of blood glucose levels or temperature.
5. May be multiple effectors and/or sensors.
6. IC (needed when there are multiple inputs) is nervous tissue or brain.
a. Major Role -- Compares current value to set point; sends appropriate message to effectors.
b. Adjustments -- IC can adjust set points and/or critical points. Why bother? Fevers & feedforward; see previous lecture.
II. Introduction to Hormones (Primarily Endocrines)
A. How to describe or classify hormones?
1. Many Possible Classification Schemes -- Hormones can be classified by effect, chemical nature, source (which gland?), target cells, etc. etc. See Topic IV (for reference) for a extensive list.
2. Today: We will look at (1) processes controlled by hormones, (2) the major hormone producing glands, (3) details for specific hormones.
B. Summary of typical hormone roles and examples. See Becker Table 14-3 (10-3) or Sadava fig. 41.5 (table 42.1) for a list of hormones by type of function (Becker) or by source (Sadava).
1. Stress response -- cortisol, epinephrine. Regulate heart rate, blood pressure, inflammation, etc.
2. Maintenance of Homeostasis -- insulin, glucagon. Regulate blood glucose/energy supplies and concentrations of substances in general. Maintain more or less constant conditions = homeostasis.
3. Regulation of episodic or cyclic events -- estrogen, insulin, oxytocin -- regulate lactation, pregnancy, effects of eating, etc.
4. Growth/overall regulation -- growth factors, tropic hormones -- regulate production of other hormones. (Note: not all GF's are endocrines.)
C. Overview of Major Glands & Hormones -- see handout 22B for overview. For a complete list see Sadava fig. 41.5 (Table 42.1)
1. Pancreas
a. endocrine gland -- secretes glucagon and insulin into blood -- These control blood sugar balance, as explained last time.
b. also exocrine gland -- secretes digestive enzymes through duct to GI tract.
c. Regulation -- secretion of glucagon/insulin controlled by blood sugar levels and by input from sympathetic (in response to stress).
2. Adrenal Medulla & Cortex See Sadava fig. 41.11 (42.10).
a. Medulla (nervous)
(1). Stimulated by nerves
(2). Derived from neural tissue; part of autonomic NS.
(3). Secretes compounds that can act as transmitters (when signal cell to cell) but act as hormones (neuroendocrines) here -- are released into the blood. Note same compound can act as a transmitter or a neuroendocrine.
(4). Produces catecholamines. Major hormone = epinephrine (adrenaline); also secretes some norepinephrine (noradrenaline). For structures see 22A.
(5). Receptors. Receptors for these hormones/transmitters are same adrenergic receptors (α & β) discussed previously.
b. Cortex (epithelial)
(1). Stimulated by a hormone (ACTH)
(2). Derived from epithelial tissue
(3). Produces steroids = corticosteroids. For structures see Sadava fig. 41.12 (42.11).
(4). Part of HT/AP axis; more details below.
3. Hypothalamus (HT)
a. Inputs: Neuroendocrine cells in HT produce hormones -- in response to 3 inputs -- neuronal, hormonal, & local conditions. (HT has sensors for some variables such as temperature, osmolarity.)
b. Outputs: To pituitary (also called hypophysis)
(1). To anterior pituitary (AP); also called adenohypophysis
(2). To Posterior pituitary (PP); also called neurohypophysis
(3). Details of Structure/hormone release -- Two parts of pituitary (AP and PP) develop and function separately; connected differently to HT.
(a). Ant. Pit. (epithelial) -- connected by portal vessel to HT.
See handout 22B and/or Sadava fig. 41.7 (42.7).
Normally, blood flows from artery → capillary bed in some tissue → vein. Does not go from one capillary bed (or organ) to another. Blood flows through separate capillary beds in parallel, not in series.
Portal vessel connects two capillary beds in 2 organs.
Hormones released from HT, travel through portal vessel direct to AP.
(b). Post. Pit. (nervous) -- Cells of HT have bodies in HT and axons/terminals in posterior pituitary. (Sadava fig. 41.6 (42.5).
(i). Release hormones (neuroendocrines) from endings (terminals) in post. pit → blood supply.
(ii). Hormones are peptides. Made in cell body, packaged in vesicles, vesicles travel down MT's to end of neurons, hormones released by exocytosis.
4
. Post. Pit. (Sadava fig. 41.6 (42.5).a. Hormones = ADH (vasopressin) and oxytocin.
(1). ADH. Affects (primarily) water retention; has 2 names because discovered twice from different effects. Details of action to be described when we get to kidney. (Works through IP3 or cAMP.)
(2). Oxytocin. Affects milk ejection, uterine contractions -- works (at least in part) through IP3 to affect Ca++ and therefore contraction
b. Origin/action of hormones: Peptides are very similar in structure (homologous = share common evolutionary origin) but bind to different (G protein linked) receptors → dif. effects.
5. Anterior Pit -- Hypothalamus (HT) / Pituitary Axis
a. HT/Ant. Pit -- 3 stages
(1). HT → hormones (releasing factors) that signal the AP
(2). AP (anterior pituitary) → tropic hormones (ACTH, LH, etc.) that signal to glands (endocrine tissue)
(3). Glands → lipid soluble hormones (steroids & TH) which control their target organs. Overall:
HT
→ releasing hormone → AP → tropic hormone → TARGET GLAND → hormone → TARGET TISSUE → action.b. Example: How HT controls adrenal cortex
HT
→ CRH → AP → ACTH → ADRENAL CORTEX → corticosteroids → TARGET TISSUES → action(1). HT secretes corticotropin releasing hormone (CRH) into portal vessel
(2.) Ant. Pit responds by secreting ACTH (adrenal cortex tropic hormone; also called adrenocorticotropin) into general circulation
(3). ACTH stimulates adrenal cortex to produces three major types of steroids = corticosteroids. For structures see Sadava 42.12 (41.11) .
(a). Glucocorticoids. Ex: cortisol -- involved in long term stress response (after epinephrine wears off) -- has multiple effects/targets; more details later
(b). Mineralocorticoids. Ex: aldosterone -- regulates salt balance (to be discussed when do kidney)
(c). Sex Steroids -- cortex produces low levels of sex hormones (both androgens and estrogens) in both sexes post puberty. That's how females get 'male' hormones and vice versa.
c. AP also → "other hormones" (GH, Prolactin, etc.) that signal to nonendocrine tissues
6. There are other glands/hormones -- the list so far is not exhaustive but covers most of the major players. See texts for complete lists.
It is worthwhile to memorize most of handout 22B in order to keep all the hormones and glands straight.
III. Details of HT/Ant. Pit. Axis
A. Hypothalamic Hormones
1. Outputs (to AP): These cells in HT release hormones from HT itself. (As vs. cells that connect to post. pit.)
a. Release hormones into portal vessel (connects two capillary beds) that goes direct to anterior pituitary. See Sadava 41.7 (41.7) and handout 22B
b. Hormones are release factors. Hormones released by HT affect production/release of other hormones by ant. pit.
c. Affect on release -- 'release factors' can be stimulatory (RH's such as ACTH-releasing hormone) or inhibitory (IH's such as prolactin release-inhibiting hormone = PIH)
d. All HT hormones (except PIH = dopamine) are peptides/proteins
2. Additional info on dopamine (DA) & related compounds = catecholamines
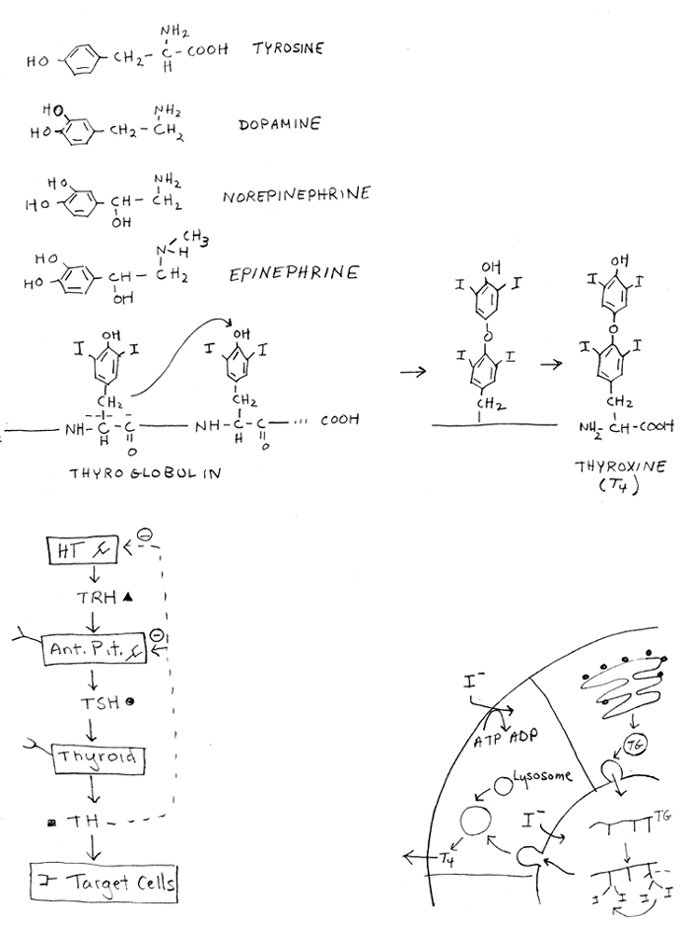
a. Structures: See handout 22A for structures of catecholamines = epinephrine (aka adrenaline), norepinephrine (aka noradrenaline), and dopamine. These are all modified amino acids derived from tyrosine. All water soluble. (Note thyroxine is also derived from tyrosine but is not a catecholamine; it is lipid soluble -- see below.)
b. Receptors: There are multiple receptors for all of the catecholamines. Receptors are classified by their ligands and response to drugs.
(1). Dopamine has its own receptors, separate from the adrenergic receptors (for epi and norepi).
(2). FYI: All adrenergic receptors bind to both epi and norepi. Some receptor types bind better to (have higher affinity for) one, some to the other, some equally well to both. Epinephrine acts mostly through beta adrenergic receptors; norepinephrine mostly through alpha adrenergic receptors.
c. Mechanism of action: All receptors for all catecholamines are G protein linked; effects of hormones on any particular cell type depend on (i) what receptors are present, & (ii) what G protein each receptor activates. Each G protein does one (or more) of the following: activate adenyl cyclase; inhibit adenyl cyclase; activate phospholipase C. See Previous lectures & problem 6-21 for examples of different responses to epi due to diff. receptors.
B. Hormones of Anterior Pituitary
1. Table of Major Hormones of AP -- details below -- see handout 22B
|
Tropic (or Pseudo-Tropic) Hormone(s) |
Target Organ |
Hormones/Secretions Made by Target Organ |
|
ACTH (adrenal cortex tropic H.) or adrenocorticotropin |
Adrenal Cortex |
Glucocorticoids, Mineralocorticoids & sex steroids* |
|
Gonadotropins -- LH (Luteinizing H.) and FSH (follicle stimulating H.)# |
Gonads |
Estrogens, androgens & progesterone* |
|
TSH (thyroid stimulating H.) or Thyrotropin |
Thyroid |
Thyroxine* |
|
GH (Growth H.) = somatotropin |
Liver (& others) |
Insulin-Like Growth Factors |
|
Prolactin |
Mammary Gland |
Milk |
* All lipid soluble hormones travel through the blood attached to plasma proteins.
#FSH stimulates Sertoli & Granulosa cells; LH stimulates Leydig & Thecal cells.
2. Tropic Hormones
a. Made by ant. pit and influence other endocrine glands. All peptides
b. Release: controlled by hormones from HT
c. Effect on target tissue
(1). Effect: Usually cause release of another hormone
(2). What is released? Hormones released by targets are steroids or act like them (thyroxine)
(3). Mechanism: All tropic hormones work through G protein linked receptors and cAMP.
(4). Question: Where are the receptors (for the appropriate hormone) on the AP? Endocrine glands? Target cells?
d. Three major tropic hormone types -- each type named after its target -- see handout 22B & table above.
See problem 7-4. (Skip choice 5 for now.)
3. Other Hormones of ant. pit.
a. GH and prolactin -- "pseudo tropic" hormones -- both peptides.
(1). Structure & mechanism: Similar in structure to each other (homologous) and use a special type of TK receptor
(2). Release: Release regulated by release/inhibitory factors from HT.
(3). What is released from target cells? Stimulate production of secretions, but not from endocrine glands.
(a). GH stimulates liver (& possibly other tissues) to produce insulin-like growth factors (ILGF 1 & 2); ILGF's from liver released into blood (act as endocrines); ILGF's from other tissues act as paracrines. (GH has other effects as well.)
(b). Prolactin stimulates mammary (exocrine) gland to produce milk. (Need oxytocin to eject the milk.)
| Hormone (from AP) | Receptor & 1st Target | Secretion by 1st Target | Final Target | |||
| Tropic Hormone | → | GPCR in endocrine gland | → | endocrine (steroid or TH.) | → | blood |
| Pseudo Tropic Hormones | ||||||
| GH (somatotropin) | → | TKR in Liver* | → | ILGFs | → | blood |
| Prolactin | → | TKR in exocrine gland | → | milk | → | outside |
* GH also effects other tissues -- some respond directly and
some make ILGFs that affect other tissues/cells. ILGFs make by tissues other
than liver are paracrines.
TKR = Tyrosine kinase receptor; GPCR = G protein coupled receptor
(4). What's the difference between endocrine & exocrine glands? See handout 12C of '08. To review:
(a). Exocrine Gland
When gland forms, epithelial layer leaves duct to outside.
Secretion from gland flows into duct → outside or lumen.
Examples:
(i) sweat, mammary & tear glands → secretion → outside
(ii) stomach glands & pancreas → secretion → lumen.(b). Endocrine Gland
When gland forms, epithelial layer pinches off leaving no duct
Secretion (hormone) from gland enters blood.
Example: gonads, pancreas, adrenal.
(c) Both types get precursors for secretions from blood
Try problems 7-1 & 7-13.
b. MSH (melanocytye stimulating H) etc.
(1). Common source: All come from cleavage of single peptide precursor (pro-opio-melanocortin or pomC) that is cut up to give ACTH and MSH etc.
(2). Alternative ways of cleavage: Same precursor can be cut up different ways in different tissues and/or species. Note: this is alternative processing of a protein, not an RNA.
(3). Function: Function of these hormones is relatively obscure. MSH may be involved in control of body weight as well as pigmentation.
(4). Protein Precursors: 'pro-hormones' & 'pre-pro-hormones':
(a). Many hormones are made as inactive precursors = pro-hormones. Example: pro-insulin.
(b). 'pre-pro-hormone' = pro-hormone with its signal peptide still attached = sequence that gene codes for.
(c). Some enzymes are also made in an inactive forms (called zymogens) -- for example, trypsinogen, fibrinogen. Zymogen or pro-hormone has amino acids that must be removed to give fully active product (insulin, typsin, fibrin, etc.).
Try Problem 7-2 & 7-4 if not yet done, but skip choice 5 (of 7-4) for now.
B. Regulation of HT/AP Axis
1. General case: See Sadava fig. 41.8 (42.8)
a. The cascade:
HT → RH → AP → tropic hormone → TARGET GLAND → hormone → TARGET TISSUE → action.
b. Regulation: Hormone from target gland (thyroxine, sex steroids, etc.) has negative feedback effect on AP (& also in some cases on HT).
2. Specific case: thyroxine production (See handout 22A)
a. The cascade:
HT → TRH → AP → TSH → TARGET GLAND → TH → TARGET TISSUE → increase in BMR, etc.
b. Regulation
(1). Negative Feedback: TH inhibits production of both TSH and TRH. (Where are the receptors? On cell surface or intracellular??) Primary effect is at AP -- reduces response to TRH.
(2). Two different types of goiter (enlarged thyroid)
(a). When TH is low (hypothyroidism): Lack of iodine or other factor → low level of TH → lack of negative feedback to HT &/or AP → overproduction of TSH → goiter. See Sadava fig. 41.9 (8th ed)
(b). When TH is high (hyperthroidism): Can sometimes still have too much stimulation of thyroid even in presence of TH. Problem can be over production of TRH and/or TSH (due to tumors, failure of feedback, etc.), or to over stimulation of TSH receptors by other factors. See Graves disease below.
(3). Graves disease = antibodies to TSH receptors act as agonists of TSH. (Case of (b) above). Reminder:
agonist = acts like -- or has same effect as -- normal ligand
antagonist = blocks action of -- or effect of -- normal ligand
c. What does thyroxine do? Raises BMR and is needed for normal alertness and reflexes. Needed during childhood for brain development.
d. How is thyroxine made & stored? By modification and rearrangement of tyrosines in thyroglobulin (TG) -- see handout 22A or Sadava 41.9 (8th ed). How is TG made & TH released from it ?
protein (TG) made on RER → Golgi → vesicles
exocytosis of vesicles releases TG into lumen
I- taken up into gland; I added to tyrosines of TG in lumen; one modified tyrosine added to OH of another.
Modified TG stored in lumen of gland = reservoir of TH
TG taken up by cell from gland by RME. Result is degradation of TG in lysosomes → releases T4 or T3 (= TH)
TH diffuses out of cell across membrane. Acts like a steroid. (For structures see handout or texts.)
TSH stimulates virtually all of these steps.
e. How does thyroxine travel through the blood? All lipid soluble hormones are attached to plasma proteins, either to general proteins or specific binding proteins for that hormone. T4 and T3 are transported by thyroxine-binding globulin, which is specific for thyroxine. Note: thyroglobulin is not the same as thyroxine-binding globulin. (Globulin just means globular, soluble protein.)
Try problem 7-5 & 7-9. (If you have time, there are additional problems on this topic -- most of problem set 7. )
IV. How
to Keep Track of Hormones
-- How to Classify Hormones & Growth Factors
(or Signal Molecules in General). The following is meant as a check list to help
you keep track of the various signal molecules. It is for reference & study
purposes; it will not be discussed in class.
Some of these questions/categories overlap, and you can't answer all
the questions for all the hormones, growth factors, etc., but the list helps to organize the information you do
have.
1. Type of Action -- Is it paracrine, endocrine (hormone), growth factor, neurotransmitter, etc.? (See handout 12B
2. Chemical nature -- Is it a peptide, amino acid or derivative, fatty acid or derivative, or steroid? See Becker table 14-4.
3. Where is it made? In what gland or tissue? (HT? pancreas?) See Sadava fig. 41.5 (Table 42.1)
4. Target Cells -- where does it act? (Muscle and liver or just liver?)
5. Mechanism of signal transduction
A. Location/type of receptor on target cells -- Is receptor on surface or intracellular? TK or G protein linked?
B. Type of signal transduction -- Is there a second messenger? Which one? If none, what links receptor to intracellular events?
C. Intracellular mode of action -- what mechanism is used to get the end result? Is there a change in enzyme activity? change in transcription? both? change in state of ion channel?
6. What actually gets done? What happens?
A. Biochemically speaking: Which target enzymes, proteins or genes are affected (glycogen phosphorylase activated? Cyclin gene transcribed?)
B. Physiological End Result: Another hormone secreted? Glycogen broken down, & Glucose in blood up? Note the "result" may have several steps, and more than one can sometimes be considered "the end."
C. What's the (teleological) point? What overall function is served by the signal molecule's action?
1. One list of possibilities: Homeostasis, response to stress, growth, maintenance of some cycle;
2. An alternative version of the list: Regulation of rates of processes, growth & specialization, Conc. of substances, and response to stress.
3. The 2 lists are really the same = homeostasis (control of rates & concentrations), response to stress, & regulation of growth (unidirectional and cyclic).
Next Time: Wrap up of TH, and then how salt and water homeostasis is maintained (kidney function).
{kind=link}
{kind=link}