Abstract
BACKGROUND: The contribution of somatic mosaicism, or genetic mutations arising after oocyte fertilization, to congenital heart disease (CHD) is not well understood. Further, the relationship between mosaicism in blood and cardiovascular tissue has not been determined.
METHODS: We developed a new computational method, EM-mosaic (Expectation-Maximization-based detection of mosaicism), to analyze mosaicism in exome sequences derived primarily from blood DNA of 2530 CHD proband-parent trios. To optimize this method, we measured mosaic detection power as a function of sequencing depth. In parallel, we analyzed our cohort using MosaicHunter, a Bayesian genotyping algorithm-based mosaic detection tool, and compared the two methods. The accuracy of these mosaic variant detection algorithms was assessed using an independent resequencing method. We then applied both methods to detect mosaicism in cardiac tissue-derived exome sequences of 66 participants for which matched blood and heart tissue was available.
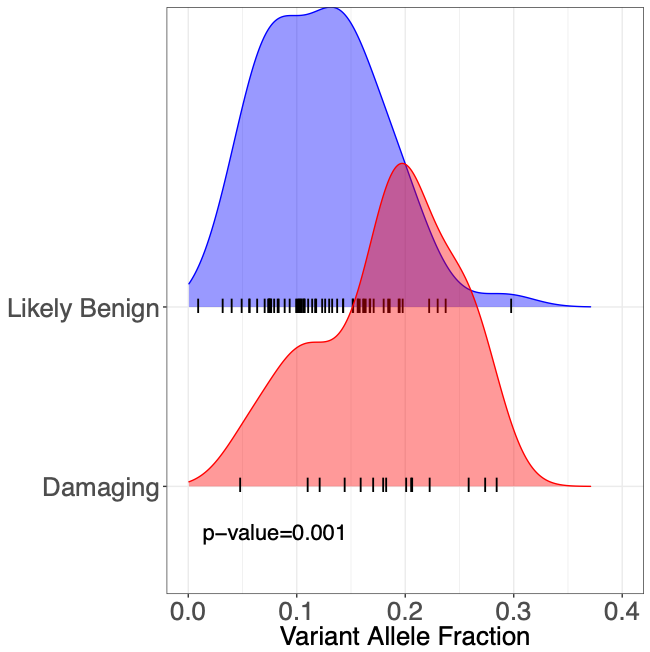
RESULTS: EM-mosaic detected 326 mosaic mutations in blood and/or cardiac tissue DNA. Of the 309 detected in blood DNA, 85/97 (88%) tested were independently confirmed, while 7/17 (41%) candidates of 17 detected in cardiac tissue were confirmed. MosaicHunter detected an additional 64 mosaics, of which 23/46 (50%) among 58 candidates from blood and 4/6 (67%) of 6 candidates from cardiac tissue confirmed. Twenty-five mosaic variants altered CHD-risk genes, affecting 1% of our cohort. Of these 25, 22/22 candidates tested were confirmed. Variants predicted as damaging had higher variant allele fraction than benign variants, suggesting a role in CHD. The estimated true frequency of mosaic variants above 10% mosaicism was 0.14/person in blood and 0.21/person in cardiac tissue. Analysis of 66 individuals with matched cardiac tissue available revealed both tissue-specific and shared mosaicism, with shared mosaics generally having higher allele fraction.
CONCLUSIONS: We estimate that ~ 1% of CHD probands have a mosaic variant detectable in blood that could contribute to cardiac malformations, particularly those damaging variants with relatively higher allele fraction. Although blood is a readily available DNA source, cardiac tissues analyzed contributed ~ 5% of somatic mosaic variants identified, indicating the value of tissue mosaicism analyses.