Abstract
Purpose: Congenital diaphragmatic hernia (CDH) is associated with significant mortality and long-term morbidity in some but not all individuals. We hypothesize monogenic factors that cause CDH are likely to have pleiotropic effects and be associated with worse clinical outcomes.
Methods: We enrolled and prospectively followed 647 newborns with CDH and performed genomic sequencing on 462 trios to identify de novo variants. We grouped cases into those with and without likely pathogenic (LP) variants and systematically assessed CDH clinical outcomes between the genetic groups.
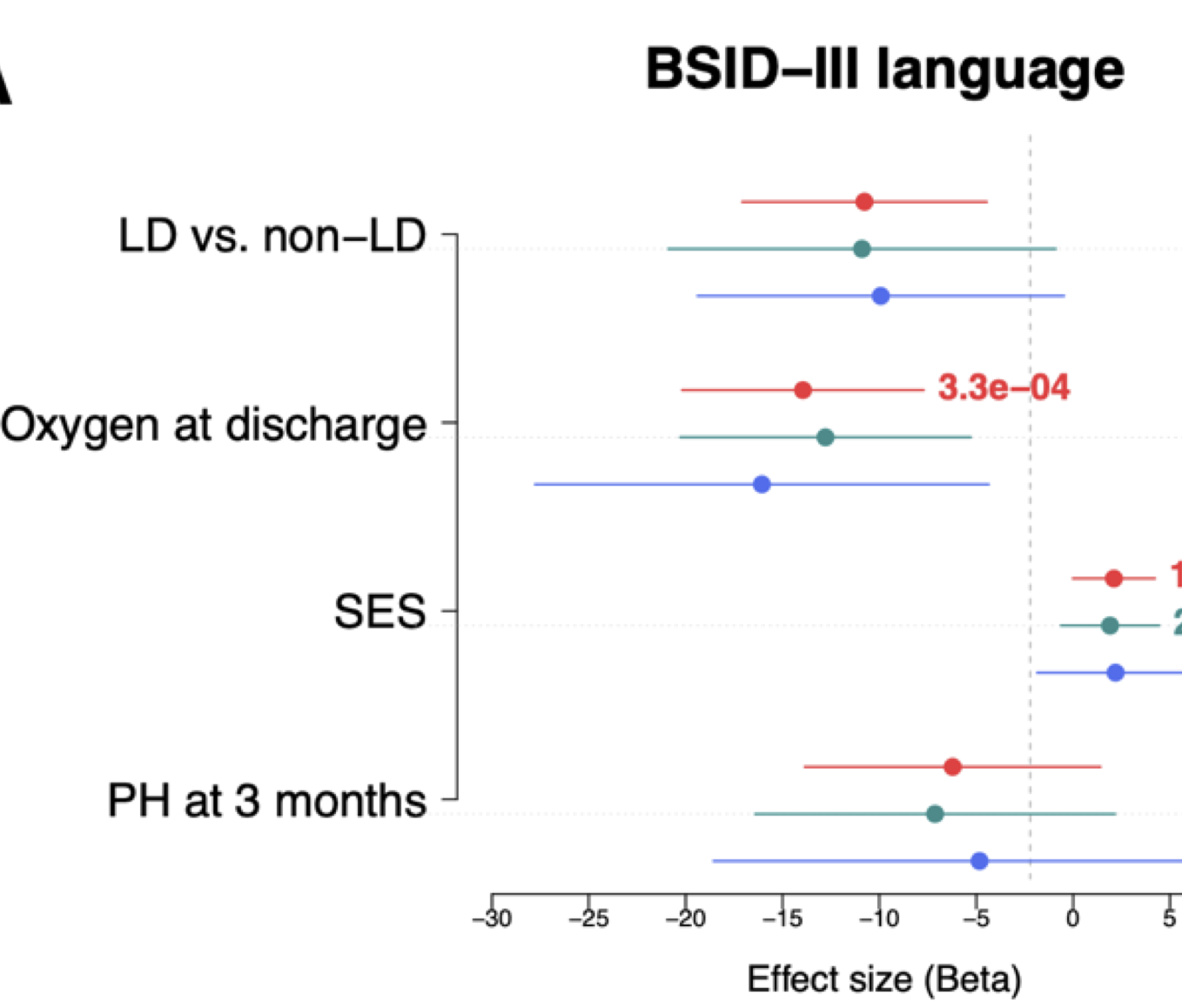
Results: Complex cases with additional congenital anomalies had higher mortality than isolated cases (P=310-6). Isolated cases with LP variants had similar mortality to complex cases and much higher mortality than isolated cases without LP (P=210-2). The trend was similar with pulmonary hypertension at 1 month. Cases with LP variants had an estimated 6-13 points lower score on neurodevelopmental assessments at 2 years than cases without LP, and the difference is similar in isolated and complex cases.
Conclusion: We found that the likely pathogenic genetic variants are associated with higher mortality, worse pulmonary hypertension, and worse neurodevelopment outcomes. Our results have important implications for prognosis and potential intervention and long-term follow up for children with CDH.