





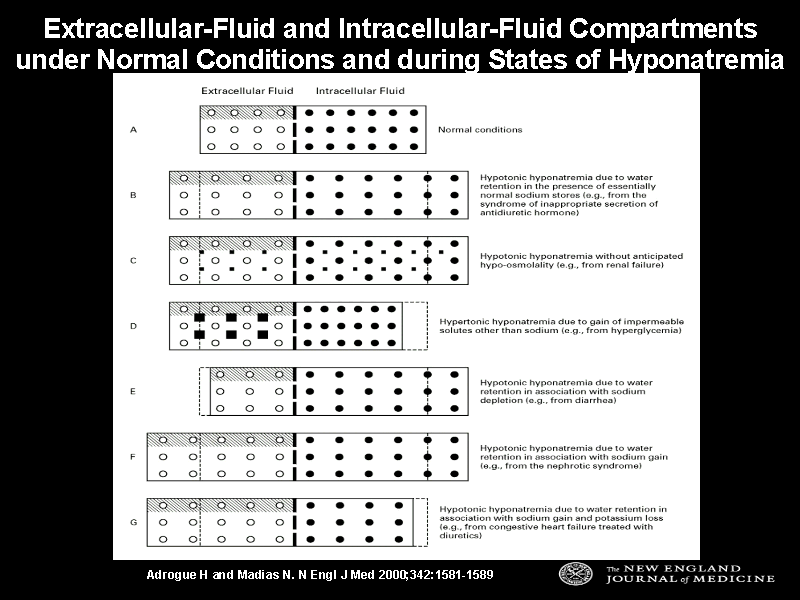
Figure 1. Extracellular-Fluid and Intracellular-Fluid Compartments under Normal Conditions and during States of Hyponatremia. Normally, the extracellular-fluid and intracellular-fluid compartments make up 40 percent and 60 percent of total body water, respectively (Panel A). With the syndrome of inappropriate secretion of antidiuretic hormone, the volumes of extracellular fluid and intracellular fluid expand (although a small element of sodium and potassium loss, not shown, occurs during inception of the syndrome) (Panel B). Water retention can lead to hypotonic hyponatremia without the anticipated hypo-osmolality in patients who have accumulated ineffective osmoles, such as urea (Panel C). A shift of water from the intracellular-fluid compartment to the extracellular-fluid compartment, driven by solutes confined in the extracellular fluid, results in hypertonic (translocational) hyponatremia (Panel D). Sodium depletion (and secondary water retention) usually contracts the volume of extracellular fluid but expands the intracellular-fluid compartment. At times, water retention can be sufficient to restore the volume of extracellular fluid to normal or even above-normal levels (Panel E). Hypotonic hyponatremia in sodium-retentive states involves expansion of both compartments, but predominantly the extracellular-fluid compartment (Panel F). Gain of sodium and loss of potassium in association with a defect of water excretion, as they occur in congestive heart failure treated with diuretics, lead to expansion of the extracellular-fluid compartment but contraction of the intracellular-fluid compartment (Panel G). In each panel, open circles denote sodium, solid circles potassium, large squares impermeable solutes other than sodium, and small squares permeable solutes; the broken line between the two compartments represents the cell membrane, and the shading indicates the intravascular volume.