Clinical Cases: Part II
Case One: Mark Guttman is a 39 year old white male living in Stamford, Connecticut. Mr. Guttman is here to see you for a follow up to an initial routine health care maintenance exam.
- Past Medical History
- None
- Not on any medications
- No known allergies
- Social History
- Smokes tobacco ¼ pack a day
- Occasional EtOH at social functions only
- No drug use
- Works as a teacher in a middle school
- Was born in Westchester County, NY and lived in Connecticut is entire life
- Single, Not sexually active currently
- Family History
- Father is alive and healthy, Age 60
- Mother has diabetes, Age 59
- No siblings or children
- Pertinent Physical Exam
- BP 135/80
- Weight 190 lbs
- Height 5’ 9”
- BMI 28.1
- Waist Circumference 38 inches
- Fasting Cholesterol Panel
- Total Cholesterol 220
- LDL 162
- HDL 38
- Triglycerides 165
What treatment strategies for hyperlipidemia should be offered to Mr. Guttman?
The correct answer is D. Mr. Guttman has 2 risk factors and a 10-year risk category of 10-20%. He should initiate and maintain therapeutic lifestyle changes (TLC) and consider adding LDL lowering drug if LDL is >130 after 3 months of TLC; you should assess for the presence of metabolic syndrome and its management after maximal response to LDL treatment.
Case Two: Maria De Los Santos is a 67 year old Dominican female living in Washington Heights. She has been your patient for 8 years and is here to discuss the results of her fasting lipid panel.
- Past Medical History
- Diabetes, Hypertension
- Meds – Metformin, Ramipril only
- No known allergies
- Social History
- Has never smoked tobacco
- No alcohol use
- No drug use
- Worked as an office administrator and retired 2 years ago
- Was born in Santiago, Dominican Republic and moved to New York City 37 years ago
- Married, and sexually active currently in monogamous relationship
- Family History
- Father is alive and has diabetes, hypertension, and peripheral vascular disease, age 87
- Mother has diabetes, age 88
- Brother has diabetes, age 65
- She has 3 adult children that are all healthy
- Pertinent Physical Exam
- BP 145/81
- Weight 210
- Height 5’ 8”
- BMI 31.9
- Waist Circumference 42 inches
- Fasting Cholesterol Panel
- Total Cholesterol 189
- LDL 115
- HDL 56
- Triglycerides 179
Aside from therapeutic lifestyle changes, should LDL lowering drug therapy be offered to Mrs. De Los Santos?
The correct answer is B. Mrs. De Los Santos has an LDL of 115 and a >20% 10-year CHD risk. According to ATP III recommendations, initiating LDL lowering drugs is an option.
Case Three: Nelson Nguyen is a 43 year old Vietnamese male living in Castro Valley, CA. He has been your patient for 5 years and is here to discuss the results of his fasting lipid panel. He had been lost to follow up to your practice for 2 years. He was taking only hydrochlorathizide (was buying it on own over past 2 years – you added a second hypertension med at the last visit)
- Past Medical History
- Hypertension
- Meds – Now taking hydrochlorathizide and a beta blocker
- Allergies - Penicillin
- Social History
- Smokes tobacco – 1 pack a day
- No alcohol use
- No drug use
- Works as a coffee shop manager
- Was born in Quy Nhon, Vietnam and immigrated to the United States at age 23
- Married, and sexually active currently in monogamous relationship
- Family History
- Father died at age 47 of unknown causes
- Mother is alive and healthy in Vietnam, age 65
- Older brother died of a myocardial infarction at age 45
- Has 2 sons that are healthy and in college
- Pertinent Physical Exam
- BP 160/90
- Weight 200
- Height 5’ 6”
- BMI 32.3
- Waist Circumference 39 inches
- Fasting Cholesterol Panel
- Total Cholesterol 272
- LDL 188
- HDL 42
- Triglycerides 202
What is Mr. Nguyen’s 10-year cardiovascular risk category?
The correct answer is E. Mr. Nguyen should initiate and maintain intensive therapeutic lifestyle changes (TLC) and initiate LDL lowering drug simultaneously; also maximal control of other risk factors should be achieved including his hypertension and smoking cessation.
STEP EIGHT: METABOLIC SYNDROME
Identify metabolic syndrome and treat, if present, after 3 months of TLC.
Clinical Identification of the Metabolic Syndrome – Any 3 of the following must be present:
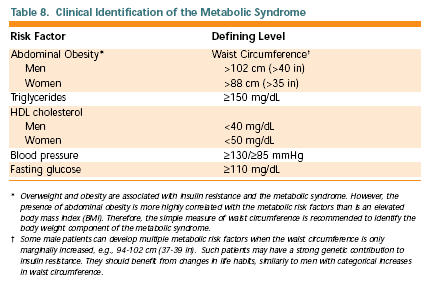

Table from Adult Treatment Panel III. Executive Summary of the Third Report
of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation,
and Treatment of High Blood Cholesterol in Adults JAMA, May 16, 2001
Treatment of the metabolic syndrome
- Treat underlying causes (overweight/obesity and physical inactivity):
- Intensify weight management
- Increase physical activity.
- Treat lipid and non-lipid risk factors if they persist despite these lifestyle therapies:
- Treat hypertension
- Use aspirin for CHD patients to reduce pro-thrombotic state
- Treat elevated triglycerides and/or low HDL
More information on metabolic syndrome is available in the library.
STEP NINE: TREAT ELEVATED TRIGLYCERIDES
ATP III Classification of Serum Triglycerides (mg/dL):
<150 Normal
150-199 Borderline high
200-499 High
≥500 Very high
Treatment of elevated triglycerides (≥150 mg/dL)
- Primary aim of therapy is to reach LDL goal
- Intensify weight management
- Increase physical activity
- If triglycerides are >200 mg/dL after LDL goal is reached, set secondary goal for non-HDL cholesterol (total – HDL) 30 mg/dL higher than LDL goal.
| Comparison of LDL Cholesterol and Non-HDL Cholesterol Goals for Three Risk Categories | ||
|---|---|---|
Risk Category |
LDL Goal (mg/dL) |
Non-HDL Goal (mg/dL) |
CHD and CHD Risk Equivalent (10-year risk for CHD >20%) |
<100 |
<130 |
Multiple (2+) Risk Factors and 10-year risk ≤20% |
<130 |
<160 |
0-1 Risk Factor |
<160 |
<190 |
If triglycerides 200-499 mg/dL after LDL goal is reached, consider adding drug if needed to reach non-HDL goal:
- intensify therapy with LDL-lowering drug, or
- add nicotinic acid or fibrate to further lower VLDL.
If triglycerides ≥500 mg/dL, first lower triglycerides to prevent pancreatitis:
- very low-fat diet (≤15% of calories from fat)
- weight management and physical activity
- fibrate or nicotinic acid
- when triglycerides <500 mg/dL, turn to LDL-lowering therapy.
Treatment of low HDL cholesterol (<40 mg/dL)
First reach LDL goal, then:
- Intensify weight management and increase physical activity
- If triglycerides 200-499 mg/dL, achieve non-HDL goal
- If triglycerides <200 mg/dL (isolated low HDL) in CHD or CHD equivalent consider nicotinic acid or fibrate.
ATP III Resources For Physicians and Students
Once you understand the principles behind the ATP III, you don’t have to memorize all these steps. Several resources are available for physicians and students that can be used during patient care:
National Cholesterol Education Program
http://www.nhlbi.nih.gov/about/ncep/index.htm
ATP III At A Glance
http://www.nhlbi.nih.gov/guidelines/cholesterol/atglance.pdf
ATP III Palm OS Interactive Tool
http://hp2010.nhlbihin.net/atpiii/atp3palm.htm
10 Year Risk Calculator
http://hp2010.nhlbihin.net/atpiii/calculator.asp?usertype=prof