Diagnosing Mood Disorders Part 3
Depression in Pregnancy and Postpartum Depression
You have a 28 year old woman who is in her third trimester of pregnancy. She has been diagnosed with severe depression and is under the care of a psychiatrist. She wants to discuss with you the risk of taking antidepressants during the rest of her pregnancy. Which of one of the following statements is true? (Choose the best answer.)
Although depression in pregnancy and postpartum depression is beyond the scope of this web module, it is important for primary care physicians to be aware of screening these patients for timely intervention.
Medical management of depressed patients during pregnancy usually stirs discomfort in physicians because of fear of teratogenic effects in the fetus. Adverse effects of not treating this population are well documented, as well as the safety profiles of commonly prescribed psychiatric medications. Selective serotonin reuptake inhibitors are the agents of choice. Fluoxetine and tricyclic antidepressants appear to have no teratogenic effects, however the Food and Drug Administration (FDA) has determined that exposure to paroxetine in the first trimester of pregnancy may increase the risk for congenital malformations, particularly cardiac malformations. The mood stabilizers (e.g., dilantin, valproic acid, carbamazepine) appear to be teratogenic. The decisions regarding the use of psychiatric medications should be individualized. The most important factor is usually the patient’s level of functioning in the past when she was not taking medications. There is a small but significant risk of “withdrawal syndrome” in the newborn if serotonergic antidepressants are taken during the third trimester. This “withdrawal syndrome” consists of irritability, inconsolable crying, tachypnea, thermal instability, and poor muscle tone but is usually mild and transient. Overall, pregnant patients, once identified with depression, should be under the care of a psychiatrist and an obstetrician or family physician with experience in high risk obstetrics. Psychotherapy has also been found to be useful in these women.
Postpartum depression typically occurs within one month of delivering a baby. Normal “baby blues” can begin 24 hours after delivery and last up to 10 days. Postpartum depression is not different from a major depressive episode, but the primary care physician or obstetrician should recognize the symptoms as immediate interventions can have positive outcomes for the mother and baby. One important challenge is that the onset of postpartum depression frequently occurs before the patient is seen for a routine six-week postpartum visit. The risk-benefit decision about whether to start antidepressants in a breastfeeding woman is based on the severity of the depression and the need for pharmacotherapy, rather than any known risks to the infant.
More information on treatment of depression in pregnancy, postpartum women, and breastfeeding woman can be found in this web module’s library.
Depression in the Elderly and Pseudodementia
Which one of the following statements is true about depression in the elderly? (Choose the best answer.)
Depression in the elderly is not part of the normal aging process. This common misconception may lead elderly patients, or their families, not to seek appropriate help. It can also lead physicians to miss the diagnosis of depression in the elderly and leave it untreated. A common complaint in elderly patients is not depression but insomnia, anorexia, and fatigue. Treatment with antidepressants, especially selective serotonin reuptake inhibitors can be useful. Patients who are elderly when they have their first episode of depression have a relatively higher likelihood of developing chronic and recurring depression. The prognosis for recovery is equal in young and old patients, although remission may take longer to achieve in older patients.
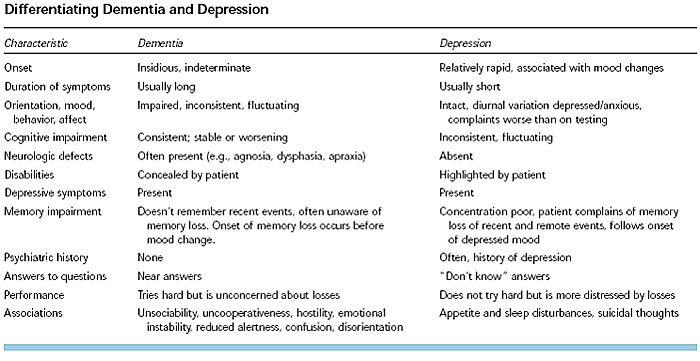
Pseudodementia, associated with severe depression, can be easily mistaken for dementia, especially in the elderly or persons with underlying neurological disease (e.g., strokes, etc). The symptoms of pseudodementia include marked psychological distress, inability to concentrate or complete daily tasks, and marked cognitive dysfunction. Differentiating between dementia and pseudodementia is important. Typically, patients suffering from pseudodementia will exhibit profound concern about their impaired cognitive function, in contrast with patients with a diagnosis of dementia, who may tend to minimize their disability. In addition to pharmacotherapy, electroconvulsive therapy may be warranted in patients with pseudodementia.
All patients with depression of all ages, including the elderly, should have a mini-mental status examination at baseline. Patients successfully treated of their major depression will see their pseudodementia and cognitive dysfunction improve.
Reproduced with permission from Birrer, R., Vemuri, S. “Depression in Later Life: A Diagnostic and Therapeutic Challenge.” American Family Physician. 2004;69:2375-82.
More information on depression in the elderly is available in this web module’s library.
Manic and Hypomanic Symptoms: Bipolar Disorder
You are evaluating a 35 year old male in your primary care practice. He has a history of depression and occasional panic attacks. His previous physicians treated his panic symptoms with selective serotonin reuptake inhibitors (SSRIs) approved for panic disorders but the medications made him more restless, agitated, and unable to sleep. Upon further questioning, you discover he has been having symptoms with impairing depressive episodes and anxiety since late childhood. His father was hospitalized with a manic episode on one occasion. Upon further exploration, which one of the following would be most specific for confirming the diagnosis of bipolar disorder? (Choose the best answer.)
A major depressive episode can appear as a unipolar disorder, but all primary care physicians should be aware that this presentation may be part of an underlying bipolar disorder. Primary care physicians who diagnose and treat patients with depression should carefully assess patients for a history or current complaint of manic and hypomanic symptoms. Misdiagnosis of a bipolar disorder patient presenting with major depressive symptoms can lead to mistreatment with antidepressants alone, which may precipitate a manic episode. A manic mood is characterized by irritability or abnormal euphoria. Hypomania can be seen as a lesser degree of mania that lasts for a shorter duration. Hypomanic patients usually can continue with their normal life routines and don’t require hospitalization. A patient with a “mixed state” has to technically satisfy all the criteria of a major depressive disorder and mania at the same time. DSM-IV criteria for mania and hypomania can be found on the next table. Patients with bipolar disorder should be referred for collaborative care with a psychiatrist.
| Summary of DSM-IV Criteria for Manic Episode |
|---|
Note: Manic-like episodes that are clearly caused by somatic antidepressant treatment (e.g. medication, electroconvulsive therapy, light therapy) should not count toward the diagnosis of Bipolar I Disorder. |
| Summary of DSM-IV Criteria for Hypomanic Episode |
|---|
Note: Manic-like episodes that are clearly caused by somatic antidepressant treatment (e.g. medication, electroconvulsive therapy, light therapy) should not count toward the diagnosis of Bipolar II Disorder. |